Coalition Appropriations Letter to Senate Subcommittee on CDC Funding for FY 2022
June 2021

June 24, 2021
The Honorable Patty Murray
Chair, Subcommittee on Labor, HHS, Education and
Related Agencies
Senate Appropriations Committee
Washington, DC 20510
The Honorable Roy Blunt
Ranking Member, Subcommittee on Labor, HHS, Education and Related Agencies
Senate Appropriations Committee
Washington, DC 20510
Dear Senators Murray and Blunt:
On behalf of the Big Cities Health Coalition (BCHC), I write to ask you to provide the highest possible funding for the U.S. Centers for Disease Control and Prevention (CDC), central to protecting the public’s health, for Fiscal Year 2022. BCHC is comprised of health officials leading 30 of the nation’s largest metropolitan health departments, who together serve more than 62 million – or one in five – Americans. Our members work every day to keep their communities as healthy and safe as possible.
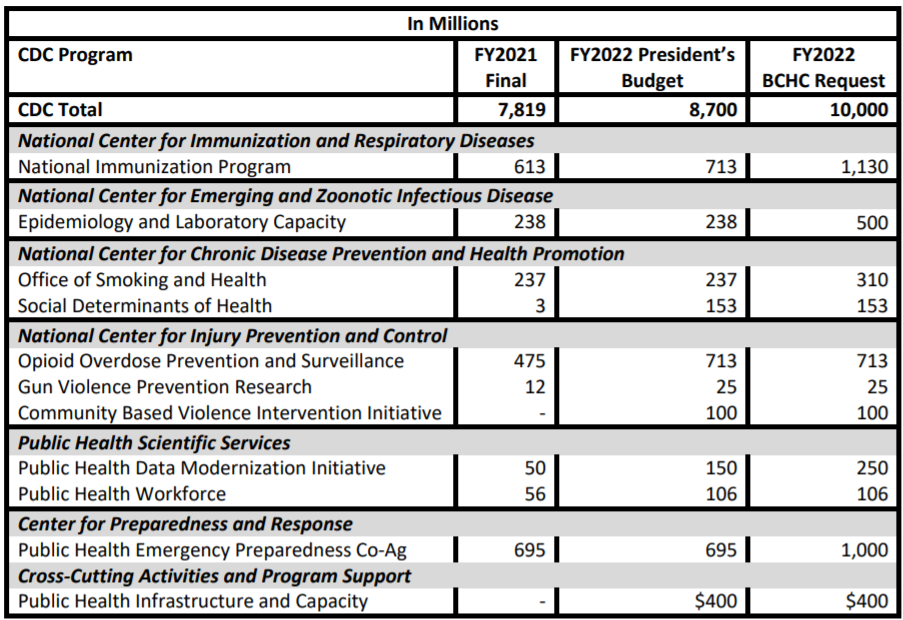
We thank you for your continued leadership and support for our nation’s public health workforce and systems during the ongoing COVID-19 pandemic. As you both recognize, federal funding for CDC and the programs that support local and state public health departments have remained largely stagnant. Additional investments through sustained annual funding is necessary to build public health capacity for the next pandemic, as well as the everyday programs. BCHC respectfully requests that you consider increases to the CDC programs listed below in the FY2022 Labor-HHS-Education spending bill.
National Immunization Program
The CDC Immunization Program funds 50 states, six large, BCHC member cities (Chicago, Houston, New York City, Philadelphia, San Antonio, and Washington, D.C.), and eight territories for vaccine purchase and immunization program operations. In addition to the challenges of the COVID-19 pandemic and continuing disease outbreaks, recent growth of electronic health records and compliance with associated regulations, new vaccines and school requirements have increased the complexity of vaccine management. Additional base funding is needed for each grantee to sustain improvements supported by emergency funding and maintain sound and efficient immunization infrastructure. We also ask that the Committee encourage CDC to be as flexible as possible in coordinating funding and guidance across immunization program streams as we move forward with COVID vaccination programs while still also carrying out routine immunizations.
Epidemiology and Lab Capacity
The Epidemiology and Lab Capacity (ELC) grant program is a single vehicle for multiple programmatic initiatives that go to 50 state health departments, six large, BCHC member cities (Chicago, Houston, Los Angeles County, New York City, Philadelphia, and Washington, D.C.), Puerto Rico, and the Republic of Palau. ELC grants strengthen local and state capacity to contain infectious disease threats by detecting, tracking and responding in a timely manner, as well as maintaining core capacity as the nation’s public health eyes and ears on the ground. Increased funding will help build the epidemiology workforce, allowing state and local health departments to begin to move towards establishing a minimum epidemiology workforce; to promote and offer training for state and local epidemiologists; and to monitor needs in state- and/or local-based epidemiology capacity. ELC dollars sent to the states should be tracked through existing CDC reporting structures and shared publicly to ensure funds are also supporting big city epidemiology activities.
Office of Smoking and Health (OSH)
Tobacco use has long been the leading preventable cause of death in the United States. Each year, it kills more than 480,000 Americans and is responsible for approximately $170 billion in health care costs. OSH has a vital role to play in addressing this serious public health problem. It provides grants to states and territories to support tobacco prevention and cessation, runs a highly successful national media campaign, conducts research and surveillance on tobacco use, and develops best practices for reducing it. Additional resources will allow OSH to address the alarmingly high rates of youth e-cigarette in addition to other forms of tobacco.
Social Determinants of Health (SDOH)
CDC’s SDOH program was initially funded in FY2021 to coordinate CDC’s activities and to begin to provide tools and resources to public health departments, academic institutions, and nonprofit organizations to address the social determinants of health in their communities. Local and state health and community agencies lack funding and tools to support these cross-sector efforts and are limited in doing so by disease specific federal funding. Given appropriate funding and technical assistance, more communities could engage in opportunities to address social determinants of health that contribute to high health care costs and preventable inequities in health outcomes.
Opioid Overdose Prevention and Surveillance
Many health departments were forced to curtail opioid and other substance use disorder prevention and related services during the pandemic. Unfortunately, overdose numbers are increasing in many communities, erasing progress of recent years. Previously, programs that connected with people in hospital emergency departments after an overdose had seen successful outcomes in steering people toward syringe services programs and treatment programs. However, these programs rely on in person interactions that have been scaled back during the pandemic. Funding is needed in local communities to ensure that substance use disorder prevention continues to stem the tide of overdose and death. We also encourage the Committee to include directive language to ensure these dollars reach the local level in those communities that are not directly funded, as well as have CDC and the Office of the Assistant Secretary of Health at the Department of Health and Human Services better track and share publicly state expenditures
Gun Violence Prevention Research
Firearm violence is a serious public health problem in the United States that impacts the health and safety of all Americans. Despite initial funding in FY 2021 to research key issues around firearm violence, significant gaps remain in our knowledge about the problem and ways to prevent it; we need to continue and expand the research. Addressing these gaps is an important step toward keeping individuals, families, schools, and communities safe from firearm violence and its consequences. The public health approach to violence prevention includes working to define the problem, identifying risk and protective factors, developing and testing prevention strategies, and then, assuring widespread adoption of effective, targeted programs. Additional funds in FY2022 could provide grants to conduct research into the root causes and prevention of gun violence focusing on those questions with the greatest potential for public health impact. The goal of this research is to stem the continued rise of firearm violence across the country to make our communities safer.
Community Based Violence Intervention Initiative
The President’s budget request includes funding for a new Community Violence Intervention initiative to implement evidence-based community violence interventions locally. BCHC whole-heartedly supports such an investment. Violence, like many public health challenges, is preventable. Yet, the majority of public investments are used to address the aftermath of violence, too often through systems that can cause further harm. Communities can be made safer when we understand the events that have led to present conditions and act on this knowledge by implementing policies and practices that address the root causes of violence. By making investments in public health strategies within communities that are most impacted by violence, cities can work across sectors to shift from an overreliance on the criminal justice system and move from reimagining to realizing community safety.
Data Modernization Initiative (DMI)
DMI is working to create modern, interoperable, and real-time public health data and surveillance systems at the state, local, tribal, and territorial levels. These efforts will ensure our public health officials on the ground are prepared to address any emerging threat to public health—whether it be COVID-19, measles, a foodborne outbreak like E. coli, or another crisis. COVID-19 exposed the gaps in our public health data systems and since then Congress has provided funding for DMI through the CARES Act and American Rescue Plan Act. These investments have been critical, but the public health surveillance systems must live beyond COVID-19 and be ready for any and all future threats. This requires long-term, sustained investment to not just build capacity at the federal and state level, but also at in cities and counties across the country.
Public Health Workforce
The public health workforce is the backbone of our nation’s governmental public health system at the county, city, state, and tribal levels. Investments must be made to build back the public health workforce, as well as attract and retain diverse candidates with diverse skill sets. These funds support CDC’s fellowship and training programs including the Public Health Associate Program and the Epidemic Intelligence Service that extend the capacity of health departments and key partners at all levels of government.
Public Health Emergency Preparedness Cooperative Agreements
The public health emergency preparedness (PHEP) grant program provides funding to strengthen local (Chicago, Los Angeles County, New York City, and Washington, D.C.) and state public health departments’ capacity and capability to effectively respond to public health emergencies, including terrorist threats, infectious disease outbreaks, natural disasters, and biological, chemical, nuclear, and radiological emergencies. PHEP funding has been cut by over 30% in the last decade. Recent events, such as the response to the COVID-19 pandemic, demonstrate the need to invest in these programs to rebuild and bolster our country’s public health preparedness and response capabilities. Our systems are stretched to the brink and will need increased and stable base funding for years to rebuild and improve. We also encourage the Committee to include directive language to insure these dollars reach the local level in those communities that are not directly funded, as well as have CDC and the Office of the Assistant Secretary of Health at the Department of Health and Human Services better track and share publicly state expenditures.
Public Health Infrastructure and Capacity
The President’s budget request includes an important new investment in core public health infrastructure and support. The pandemic exposed the deadly consequences of chronic underfunding of basic public health capacity. Because public health is largely funded by disease or condition, there has been little investment in cross-cutting capabilities that are critical for effective public health. These capabilities include: public health assessment; preparedness and response; policy development and support; communications; community partnership development; organizational competencies; accountability; and equity. Governmental public health infrastructure requires sustained investments over time, and we believe this is an important start. This investment is critical to ensuring that our governmental public health system is prepared for the next pandemic as well as to strengthen the health of our communities every day.
In closing, thank you for your continued support of governmental public health programs. As you craft the FY2022 Labor-HHS-Education bill, we urge consideration of these funding recommendations for programs that are so critical to the public’s health and safety. Please do not hesitate to contact me (juliano@bigcitieshealth.org) for additional information.
Sincerely,
Chrissie Juliano, MPP
Executive Director
Big Cities Health Coalition